Artificial Intelligence and the Gartner Cycle: Time to Introduce in Undergraduate Medical Education
By Ikram Ali Burney1, Nisar Ahmed2Affiliations
doi: 10.29271/jcpsp.2024.03.253Artificial intelligence (AI) is fast getting integrated into clinical medicine and has received a lot of attention recently, after generative AI stormed its way into daily practice in November 2022.1 The age-old model of patient care (doctor-patient relationship) has found a partner in the form of machines and technology.2 Digital technology is regarded to have the potential to improve the quality of life for populations around the world.3 AI, defined as the use of machines, programmed to develop cognitive functions for learning and solving problems, can augment human intelligence and is getting integrated into medical practice rapidly. Using machine learning (ML) technology, AI can perform complex tasks such as speech-recognition, and pattern identification, such as interpretation of electrocardiogram (ECG), plain radiographs, computed tomography (CT) scans, magnetic resonance imaging (MRI), images of skin, intestine, and eye, and histopathology slides. Alternatively, using deep learning (DL) technology, AI can help with clinical reasoning, decision-making, and translation from one language to another. More recently, the large language models (LLM) have been instrumental in even problem-solving and text-generation.1,4
It is suggested that this is the appropriate time to introduce AI in the undergraduate medical curricula and the postgraduate clinical programmes, and this suggestion is also reflected in the Gartner cycle.5 Gartner cycle describes the stages of adoption and maturity of new technologies in five phases: technology transfer, peak of inflated expectations, trough of disillusionment, slope of enlightenment, and plateau of productivity.
We believe that AI in clinical medicine has reached the ‘slope of enlightenment’ and that the ‘plateau of productivity’ seems around the corner. AI is already being used in the interpretation of radiological images, diagnosis of skin pathologies, retinopathy, drug discovery, and precision oncology.6 The use of AI is also being leveraged in the fight against infectious diseases.7
Chatbots, such as ChatGPT are sceptical but increasingly being used for medical report writing.8 More recently, ChatGPT passed the US licensing examinations, performing close to the passing threshold, and demonstrated a high level of concordance in its explanations.9 The New England Journal of Medicine has established the ‘AI in Clinical Medicine’ series.6 Hence, the final part of Gartner’s cycle, the ‘plateau of productivity’ seems around the corner.
While AI is making significant strides in clinical practice, it is imperative that medical education must keep pace with the technological advances to produce doctors conversed with, and competent in the use of the technology. Literature on AI in medical education has begun to emerge. Association of Medical Education in Europe (AMEE) has produced a guide, introducing the impact of AI on medical educators and on medical education’s methods and content.10
To study the developments, and the pattern of literature on the applications and possible limitations of the use of AI in undergraduate medical education, a bibliometric analysis was carried out. Published articles on AI, either describing the integration of AI or ML in undergraduate medical curricula or exploring the perceptions of medical students, were extracted from the SCOPUS database using the keywords, “artificial intelligence” OR “machine learning” AND “medical curriculum”, OR “medical students”, OR “medical education”, OR “medical school”, OR “medical college” in the title, abstract, and keywords of all documents. Articles describing AI or ML, but not directly related to teaching in undergraduate medical programmes, were excluded. Of the 1,572 articles published till 31st December, 2021, 132 articles were included in the final analysis, which revealed a sharp increase in number of published articles from 2018 onwards (Figure 1).
One explanation for this sudden and sharp increase in interest in the subject could be the resolution of the World Economic Forum passed in 2016, leading to an increased awareness and adoption of AI in medicine, and the resultant surge in publications.11 A breakup of published literature on AI in undergraduate medical education is shown in Figure 2.
Almost 70% of the articles described the use of AI in medical education, assessment, and curriculum planning. Several articles described AI/ML tools to assess students and provide feedback across a range of skills, including surgical skills, clinical reasoning skills, and assessment of written material. Automated surgical skills assessment using accelerometer data was correlated with video analysis and was shown to be superior in assessing surgical skills of suturing and knot tying.12 Automated systems could help save expert’s time and improve training efficiency. An automated essay scoring (AES) system was employed to assess constructed-response tasks, ranging from short-answer tests to essay questions.13 AES was shown to complement the use of selected-response testing and provided medical students with detailed feedback as part of the formative assessment. Yet, another example was the application of ML to Assess Surgical Expertise (MLASE) checklist to review manu-scripts related to surgical expertise in virtual reality simulation.14
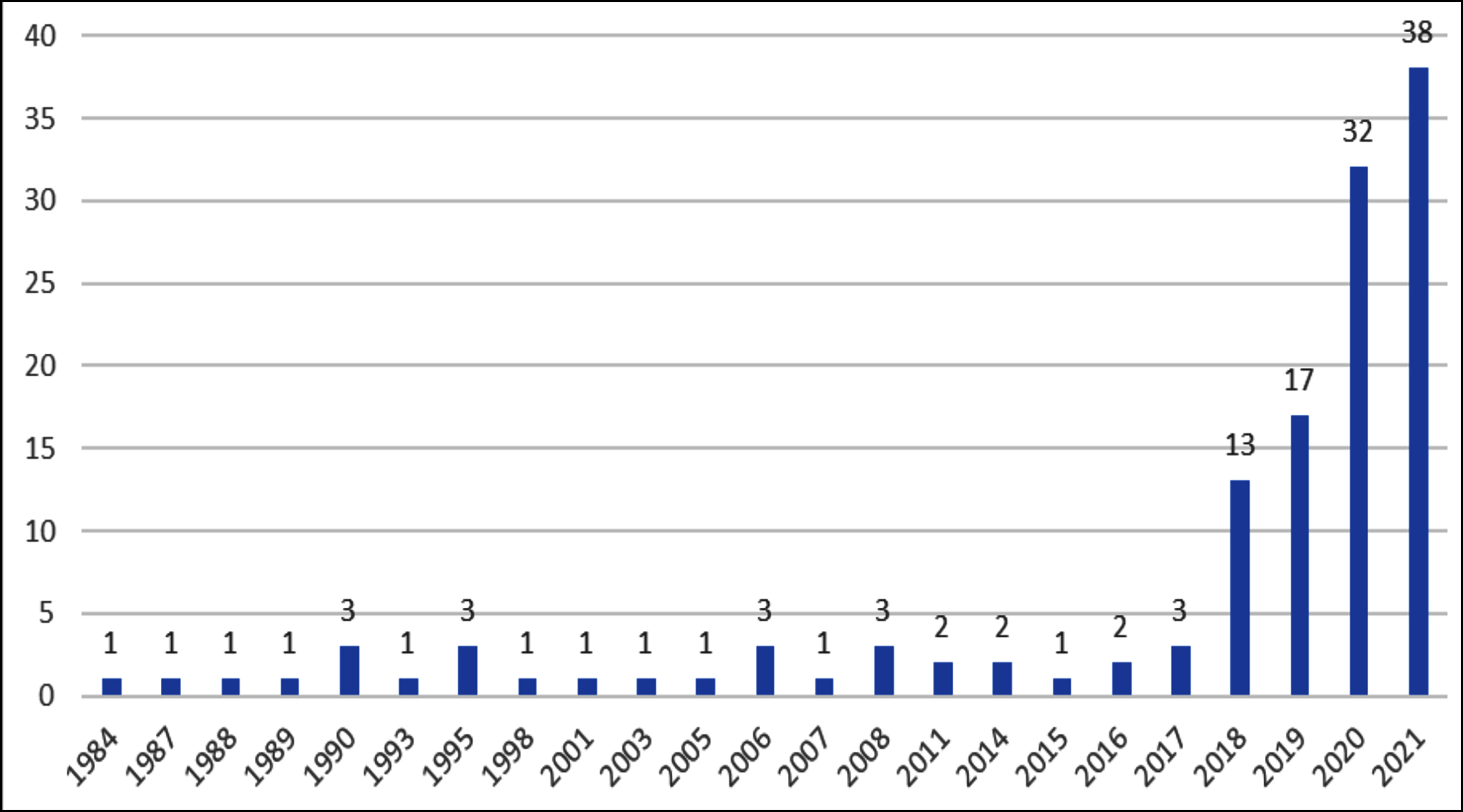 Figure 1: Number of published articles since 1984.
Figure 1: Number of published articles since 1984.
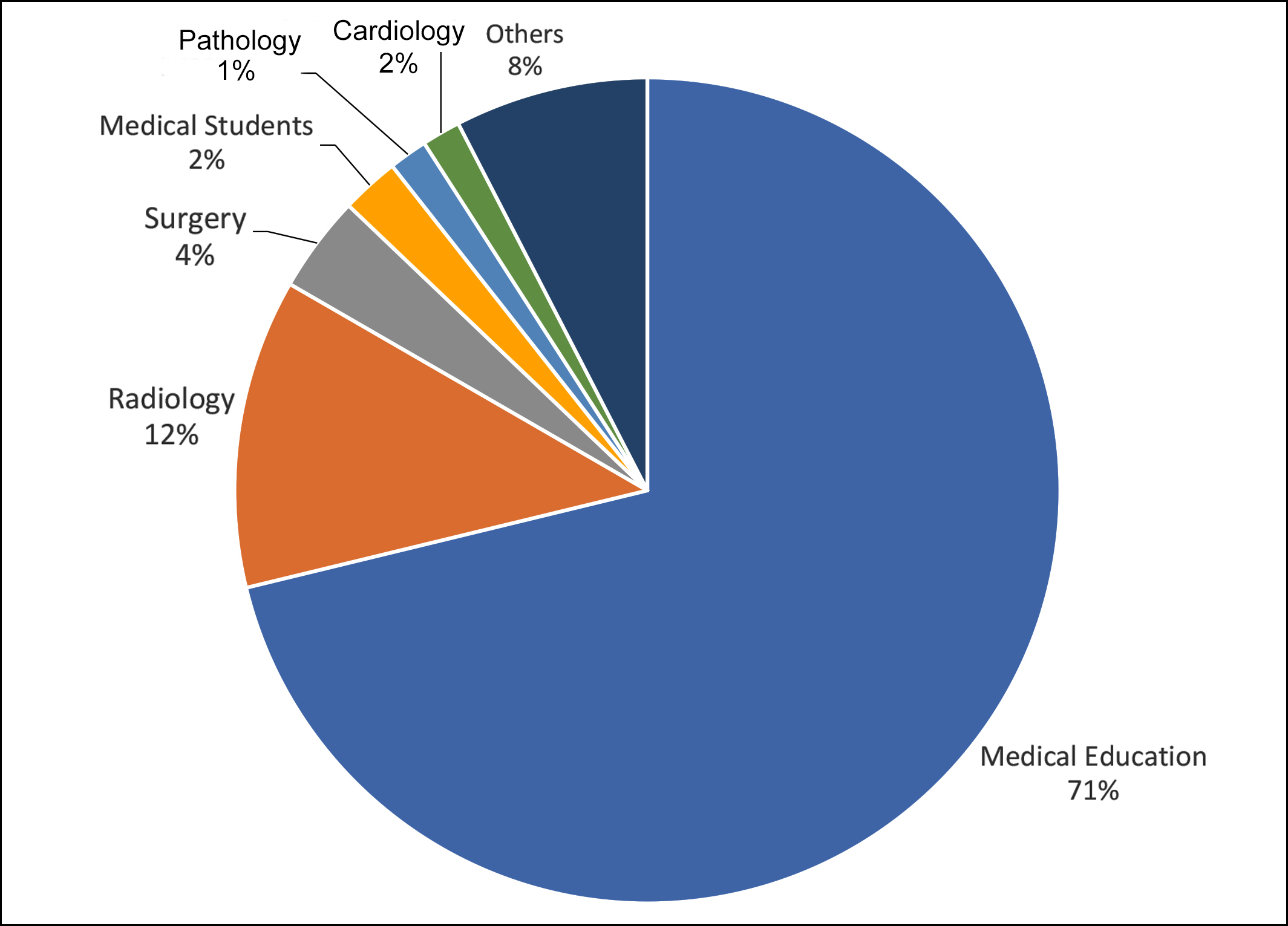 Figure 2: Pie chart showing distribution of articles according to subject matter. “Others” include one each of Dermatology, Genetics, Physiology, Psychiatry, Dental Health, Critical Care, Anatomy, and Laboratory Medicine. Articles related to medical students included the use of machine learning to identify patterns of high-risk drinking, and suicide amongst medical students.
Figure 2: Pie chart showing distribution of articles according to subject matter. “Others” include one each of Dermatology, Genetics, Physiology, Psychiatry, Dental Health, Critical Care, Anatomy, and Laboratory Medicine. Articles related to medical students included the use of machine learning to identify patterns of high-risk drinking, and suicide amongst medical students.
Besides the use of AI in medical education, a significant portion of literature centred around exploring the knowledge, perceptions, and attitudes of medical students and residents towards the use of AI in medicine. Medical students and junior doctors, especially in areas such as radiology, were cognizant of the importance of AI and saw it both as a friend and a foe. At least 10 studies explored the knowledge of undergraduate medical students of AI, their perceptions about the use of AI in the field of radiology, and their apprehensions about pursuing radiology as a career. Whereas, the majority of the interviewed students were aware of the discussion of the use of AI in radiology, a significant number expressed the need for further information about the potential use of AI in radiology.15 About 50% thought that AI was diagnostically superior and between 25 and 50% felt threatened and felt that AI might replace them in radiology.
Medical students express their desire to understand technology better and even wish to learn the use of technology in their formative years. AI is unlikely to replace clinicians, but once the tools are integrated into the clinical flow, clinicians with AI skills will have an advantage over clinicians without the skills. Competencies that medical graduates should acquire during their studies may include the basic concepts and terminology of AI, statistics, data science, awareness of functions and features of AI-related tools and applications, organising workflow in accordance with the work logic of AI, knowledge of areas where AI applications can offer healthcare solutions, and the awareness of the legal and ethical norms, and technical difficulties.16 Advancements in generative AI require medical curricula to adapt skills such as digital literacy, critical thinking, evidence-based practice, interpersonal collaboration, and continuous professional development.17 The doctors of tomorrow need to be experts not only in the biomedical and clinical sciences but also need to be able to deal with the interface between medicine and machines.
Medical education needs to keep pace with changes in medical practice. As the doctors of tomorrow need to be well-versed to be able to function better, they also need to be aware of the challenges related to technical, ethical, and legal issues, such as the dependence of AI on the data on which algorithms are developed, issues related to intellectual property rights, propagating wrong or fake facts, wrong or early versions of documents being available freely, and copyright lawsuits, to mention a few. Also, the need for the ever-important human touch in clinical medicine 'warm hands' and demonstration of empathy need to be stressed. Introduction of AI in medical curricula will help both medical professionals, as well as the medical students, to understand the concept and applications of AI to maximise its use.
REFERENCES
- Introducing ChatGPT (openai.com). https://openai.com/blog/ chatgpt.
- Snyder CF, Wu AW, Miller RS, Jensen RE, Bantug ET, Wolff AC. The role of informatics in promoting patient-centered care. Cancer J 2011; 17(4):211-8. doi: 10.1097/PPO.0b0 13e318225ff89.
- Goy A, Nishtar S, Dzau V, Balatbat C, Diabo R. Health and healthcare in the fourth industrial revolution: Global Future Council on the future of health and healthcare 2016-2019: World Economic Forum 2019. Available from: https://apo. org.au/node/235506.
- Jiang F, Jiang Y, Zhi H, Dong Y, Li H, Ma S, et al. Artificial intelligence in healthcare: Past, present and future. Stroke Vasc Neurol 2017; 2(4):230-43. doi: 10.1136/svn-2017- 000101.
- Gartner hype cycle. Gartner Hype Cycle Research Metho-dology | Gartner. Available from: https://www.gartner.com/ en/research/methodologies/gartner-hype-cycle
- Haug CJ, Drazen JM. Artificial intelligence and machine learning in clinical medicine, 2023. N Engl J Med 2023; 388(13):1201-8. doi: 10.1056/NEJMra2302038.
- Wong F, de la Fuente-Nunez C, Collins JJ. Leveraging artificial intelligence in the fight against infectious diseases. Science 2023; 381(6654):164-70. doi: 10.1126/science. adh1114.
- Lee P, Bubeck S, Petro J. Benefits, limits, and risks of GPT-4 as an AI Chatbot for medicine. N Engl J Med 2023; 388(13): 1233-9. doi: 10.1056/NEJMsr2214184.
- Kung TH, Cheatham M, Medenilla A, Sillos C, De Leon L, Elepaño C, et al. Performance of ChatGPT on USMLE: Potential for AI-assisted medical education using large language models. PLOS Digit Health 2023; 2(2):e0000198. doi: 10.1371/journal.pdig.0000198.
- Masters K. Artificial intelligence in medical education. Med Teach 2019; 41(9):976-80. doi: 10.1080/0142159X.2019. 1595557.
- Burney IA, Ahmad N. Artificial Intelligence in Medical Education: A citation-based systematic literature review. JSTMU 2022; 5(1):43-53. doi:10.32593/jstmu/Vol5.Iss1.183.
- Zia A. Automated benchmarking of surgical skills using machine learning: Georgia Institute of Technology. Int J Comput Assist Radiol Surg 2017; 13(2). doi:10.1007/ s11548-018-1735-5
- Gierl MJ, Latifi S, Lai H, Boulais AP, De Champlain A. Automated essay scoring and the future of educational assessment in medical education. Med Educ 2014; 48(10):950-62. doi: 10.1111/medu.12517.
- Winkler-Schwartz A, Bissonnette V, Mirchi N, Ponnudurai N, Yilmaz R, Ledwos N, et al. Artificial intelligence in medical education: Best practices using machine learning to assess surgical expertise in virtual reality simulation. J Surg Educ 2019; 76(6):1681-90. doi: 10.1016/j.jsurg.2019.05.015.
- Pinto Dos Santos D, Giese D, Brodehl S, Chon SH, Staab W, Kleinert R, et al. Medical students' attitude towards artificial intelligence: A multicentre survey. Eur Radiol 2019; 29(4):1640-46. doi: 10.1007/s00330-018-5601-1.
- Çalışkan SA, Demir K, Karaca O. Artificial intelligence in medical education curriculum: An e-Delphi study for competencies. PLoS One 2022; 17(7):e0271872. doi: 10. 1371/journal.pone.0271872.
- Jamal A, Solaiman M, Alhasan K, Temsah MH, Sayed G. Integrating ChatGPT in medical education: Adapting curricula to cultivate competent physicians for the AI era. Cureus 2023; 15(8):e43036. doi: 10.7759/cureus.43036.